Protocole de chromothérapie auriculaire pour le traitement du trauma psychique
- mai 27, 2026
- Com 0
Auteurs : Dr. Daniel Asis (anesthétiste, algologue), Santa Fe, Argentine ;
Dr. Alexandre Yoshizumi (acuponcteur (CMAESP)), São Paulo, Brésil;
Dr. Fabiola Luz, PhD (psychiatre, acuponcteur (CMAESP)), São Paulo, Brésil
Abstract :
The Auricular Chromotherapy has been shown promising results in the treatment of psychological trauma (PTSD).
With its relatively easy and quick technical application, and the good results produced, this procedure may be an indispensable tool for physicians.
However, its mechanism of action is not completely understood yet.
This work mentions the steps followed from the preliminary ideas about the issue to the first application in 30 patients in Santa Fé (Argentina), where the technique was created (Asis, Zarragoicoechea, 2006);
the results of 50 cases seen in São Paulo (Brazil): 41 women, 9 men, aged 20 to 60, with a 92% of success rate; and suggest some possible lines of research for the future.
Résumé :
La Chromothérapie Auriculaire, présente des resultants prometteurs dans le traitement du traumatismes psychologique . Grâce à la relative facilité et rapidité de son application technique et aux bons resultants obtenus, cette procedure peut se révéler indispensable aux médecins d’aujourd’hui.
Son mécanisme d’action n’est pourtant pas entièrement compris. Ce travail décrit les différentes étapes depuis les premières idées sur le sujet, jsuqu ‘à la première application sur 30 patients à Santa Fe, où la technique a été mise en place (Asis, Zarragoicoechea, 2006).
De plus, il presente le résultat de 50 traitements effectués à São Paulo: 41 femmes, 9 hommes, de 20 à 60 ans, avec 92% de résultats positifs. Il suggère enfin quelques lignes possibles pouvant diriger les recherches dans l’avenir.
Introduction
In PTSD (DSMIV-R, 1994), individuals develop a group of symptoms in the aftermath of a severe emotionally traumatic event.
The cardinal triad of clinical features includes: re-experiencing phenomena (e.g., flashbacks, with can occur spontaneously or in response to reminders of the traumatic event), avoidance (e.g., avoiding situations that remind the individual of the traumatic event) and hyperarousal (e.g. exaggerated startle response). Although the etiology of PTSD is defined in terms of traumatic event, evolving models of pathogenesis take into account the potential interaction between the identified traumatic event (or events), past experiences, and intrinsic individual vulnerabilities. (Rauch, S.L. et al, 2006).
It has been hypothesized that PTSD is characterized by exaggerated amygdale responsivity; abnormal activation and reduced hippocampus volume; the rostral anterior cingulated cortex is hyporesponsive and initial evidence suggest that the dorsal anterior cingulated cortex may be hyperactive (Shin, L.M. &Handwerger, K., 2009).
One important fact is that aversive events are extremely well remembered. The memory enhancement is evidently beneficial for survival, but it may become maladaptative and culminate in mental disease such a posttraumatic stress disorder. (Henckens, M.J.A.G., & cols.,2009).
Researchers found that the memory recovered is not necessarily true in details (Levine, P.A.,1999), though it is the trigger of the symptoms that come in sequence.
According with recent researches, there is good evidence that trauma-focused psychological treatments, e.g. ‘Eye Movement Desensitization and Reprocessing (EMDR)’) are more effective than those that do not focus on the patient trauma memories. (Ehlers, A &cols., 2010).
Neurophysiological findings say that anxiety is closely associated with a functional imbalance between the right and left hemispheres of the brain. (Dilts, R. &cols., 2001).
In EMDR therapy, patients are instructed to follow the therapist´s finger ith their eyes, moving them to left and to right, meanwhile activate a disturbing memory, evoking emotions, body sensations and thoughts associated with it. This bilateral stimulation also may be done tapping on client´s knees and hands, or using alternating sounds, stimulating each side alternately (Lu, D.P. & cols, 2010).
Recent studies have reported that 84 to 100% of single trauma victims no longer maintain the posttraumatic stress disorder diagnosis after the equivalent of three 90-minute sessions (Shapiro, 1999).
Auricular Chromotherapy in the treatment of psychological trauma, was created by Dr. Daniel Asis and Dr Federico Zarragoicoechea. With the contribution of Dr. Jorge Boucinhas (Brazil), and Dr. Raphäel Nogier (France). The formulation of this technique was a combination of at least three different areas of knowledge: Psychological trauma, Auriculotherapy and Chromotherapy.
The steps of this procedure began after learning ‘Eye Movement Desensitization and Reprocessing (EMDR)’ in 1997 and after having several years of practice on Auriculotherapy. We proved (using a double blind study), along Dr Gabriel Romeu, that pain relief is possible by bilaterally stimulating several points of the external ear by touch. We observed people with cervical or lumbar pain without irradiation to the limbscould be treated by simulating both ears with soft touches using the fingers. This ‘auricular tapping’ lasted 3 minutes and significantly decreased the reflex corresponding to the area called the ‘line of the psychological conflicts’ (Nogier, R.,1993) which corresponds to the Limbic area. This area will be very sensitive and painful to the touch when the person has emotional trauma. In Auriculotherapy the lobe represents the CNS.
In treatment of EMDR, the palpation of both lobes in people with emotional trauma is painful, being more painful in the left ear when the incident was more than 6-8 months ago. After the session, when the trauma was processed, the intensity of pain in these areas decreased. The alternated touch of the lobes with soft tapping in these people, similar to EMDR, doesn´t show any side effects, even when we see an acceleration of the reprocess.
Chromotherapy, or color therapy is an alternative medicine therapy whose therapists use color and light to balance physical, emotional or mental diseases. The body has different microsystems (feet, hands, cranial area and finger) similar to the external ear, the field of Auriculotherapy.
According to Dr. Boucinhas, disciple of Mandel (1997), it has been shown that the application of a specific color of radiating light to the little finger can alleviate neck pain and release restriction of movement.
The same result was seen when areas of the finger were colored with a yellow pen. Small and weak stimuli with color generating a great response of the organism, via the CNS, are based on the Arndt-Schult law (wich states: weak stimuli activate physiological processes, very strong stimuli inhibit physiological responses) and can be replicated in other microsystems.
Based on this we studied the effect of laser and yellow pen applied to hippocampus, amygdala, and ‘psychic scar’ areas (Nogier, op.cit) in relation to the treatment of emotional trauma and EMDR.
The question guide was: ‘what would happen if we applied a laser light or yellow marker in the same area as stimuli?’ The following step was to ask the patient to keep the image of the trauma, while the point was marked with a yellow fiber pen.
The response was: the image disappeared completely after one minute and at the same time the unpleasant emotions connected to the image also decreased (anguish, sadness). Dr. Frederico Zarragoicoechea replicated the technique with the same response in many patients, adding new observations. Afterward we created the protocol (see below).
Preliminary work :
In Santa Fe, Argentina, 2003, a great flood devastated 1/3 of a population who lost homes, possessions, and family members. Many years later, some people affected by the natural disaster came to Dr.Asis for different issues: chronic pain and other emotional symptoms. He began to treat them for PTSD, with the new technique that consisted of asking the patient to remember the traumatic event while the resulting sensitive part of the lobe was marked with yellow fiber pen.
In more than 30 the patients treated all experienced that after one minute the traumatic image disappeared completely while simultaneously the unpleasant emotions (anguish and sadness) and emotional pain decreased significantly.
Furthermore, a follow up survey a year later showed that 80% of patients treated were unable to reproduce the image of trauma and the associated emotional pain.
Material and method
All 50 patients were seen, and filmed using a PC camera, in the same place, at Dr. Yoshizumi´s office.
The patients were seated in a chair, in front of the camera.
One pointless pen was used to look for the sensitive ear points which were marked with yellow fiber pen.
The sessions lasted about 30 minutes.
The social classes of the patients treated were indeterminate.
All subjects of sample had attended higher learning institutions.
All of them were Dr. Yoshizumi´s patients, and 60% knew the doctor just in the day of applications.
Procedure
We used the ‘Asis and Zarragoecoechea protocol’, as follows:
AURICULAR CHROMOTHERAPY PROTOCOL FOR THE TREATMENT OF PSYCHOLOGICAL TRAUMA
Both lobes are palpated, in order to find the most painful points or two points that might be painful.
Then the patient is asked to close the eyes and to try to remember the most terrible image of the trauma, at least for one minute.
After that, the patient is asked to tell which emotion accompanies the image (is it anxiety or sadness), and describe the intensity of this emotional perturbation, on a scale of 0 to 10, which is called the SUDS Scale (Subjective Units Stress).
The patient will tell, which negative words or thoughts accompany the image, for example « I will never overcome his/her death » (Negative Cognition).
The patient is asked, which body sensation links with the emotion (oppression in the chest, for example).
The positive points will be detected using a pressure probe (painful points), electronic detection, or using the pulse, on the antitragus and the border.
The points will be colored with a yellow pen (2 – 3 points) and the patient is asked to maintain the traumatic image in mind.
The expression on the face, respiration and gestures will be observed.
Then wait for 2 minutes, and ask the patient to describe the image, generally, the image will disappear.
Measure once again with the help of the SUDS scale, which willgive a very low score (0 – 2).
Then the patient is asked, which Positive Cognition or Positive word accompanies the new (disappeared) image (« I can overcome his/her death » for example ex.).
Observe if any disturbing body sensation remains.
Results :
The distribution of trauma reasons/number according gender was as follows:
Fig. 1
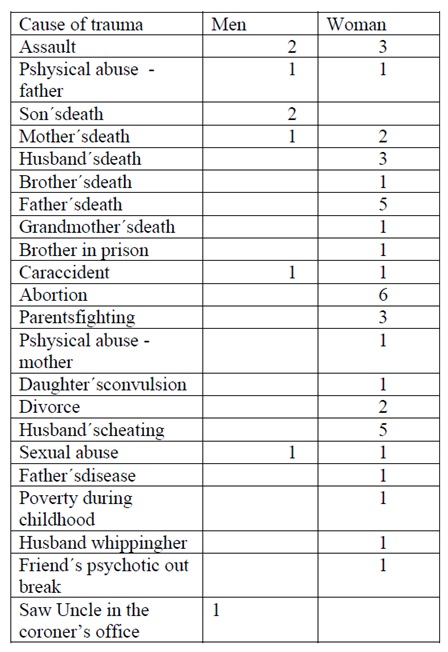
Concerning the outcomes, 46 patients reported that the traumatic image and emotional pain connected with it was erased completely or almost completely. And 4 of them reported no deleted image ( 1 ♀ traumatized by brother in prison; 1♀ suffering after and abortion; 1♀ traumatized by fighting with her husband; 1 ♂ traumatized by a car accident) but all of them with a failure response said to have felt a little bit better after treatment. In short, this is 92% positive response.
Discussion :
Despitethese encouraging results, we must take into account some points when replicating this
experiment in the future: the short sampling and the homogeneity of the cultural class could have distorted
the positive results. Another point to consider is the percentage of women present in the sampling. This
could show greater female vulnerability in suffering trauma which would be one special issue to explore at
another time. One more thing to check is the necessary follow up to cases during the years to check the
maintenance and the good effects of the treatment.
Conclusion
Upon concluding this work we have realized that this procedure shows the possibility to draw a path from the external ear to the memory center in the brain; and to apply, from the lobe, one kind of dressing, by color, on the emotional wound ‘living’ in the amygdala. These findings open space other similar experiments connecting the brain diseases with external ear, depending on the confirmation future researches can bring.
Bibliography
Asis, D.& cols. (2009) Cromo-Psicoterapias – cromoterapia auricular, Cromo-TIC, Anteojos Cromoterapeuticos. Ediciones Lux, Santa Fe.
Dils, R., Andrea C, Klein R. (2001) Eye Movement Integration. In: Aim Seminars Teaching Manual. Silver Spring, MD: American Hypnosis Training Academy. DSM-IV. Transtorno de Estresse Pós-Traumático (1995).Editora Artes Médicas. Porto Alegre.
Ehlers, A; Bisson, J; Clark, D. M. & cols. (2010) Do all psychological treatments really work the same in posttraumatic stress disorder? Clinical Psychology Review 30; 269-276.
Foa EB, Keane TM, Friedman MJ (2000): Effective Treatments for PTSD: Practice Guidelines From the International Society for Traumatic Stress Studies. New York, Guilford..
Levine, P. A. (1999)O Despertar do Tigre – Curando o Trauma. Summus Editorial.São Paulo.
Leclerc, B.(1996) Auriculothérapie théorique et pratique. Ed. Nouvelle Imprimerie Laballery.
Lu, D.P. (2010)Using alternating bilateral stimulation of eye movement desensitization for treatment of fearful patients. General Dentistry, May/June www.agd.org.
Mandel P (1997): ‘Colour puncture Compendium vol I’. New Edition.
Menon, S. B. and C. Jayan(2010) Eye Movement Desensitization and Reprocessing: A Conceptual Framework. Indian J Psychol Med. Jul-Dec; 32 (2): 136-140.
Nogier, R. (1993) Introduction pratique à l´Auriculomédecine. Ed. Haug.
Pablo y Raquel Solvey(2007) Terapias de Avanzada. RV Ediciones.
Rauch, S.L. & cols. (2006)Neurocircuitry Models of Posttraumatic Stress Disorder and extinction: Human Neuroimaging Research – Past, Present, and Future. Biol Psychiatry 60: 376-382.
Samara, Z.; Elzinga, B. & cols. (2011)Do horizontal saccadic eye movements increase interhemispheric coherence? Investigation of a hypothesized neural mechanism underlying EMDR. Frontiers in Psychiatry, 2, 1-9.
Schofferman J, Anderson D, Hines R, Smith G & Keane G (1993) Childhood psychological trauma and chronic refractory low-back pain. Clinical Journal of Pain, 9, 260-265.
Schneider, J., Hofman, A., Rost, C., Shapiro, F. (2006). EMDR in the treatment of chronic phantom limb pain. Pain medicine. American Academy of Pain Medicine.
Shapiro, F. (1999) Eye Movement Desensitization and Reprocessing (EMDR) and the Anxiety Disorders: Clinical and Research Implications of an Integrated Psychotherapy Treatment. Journal of Anxiety Disorders, Vol. 13. No. 1-2, pp. 35-67.
Shin, L.M. &Handwerger, K. (2009) Is Posttraumatic Stress Disorder A Stress-Induced Fear Circuitry Disorder?Journal of Traumatic Stress, Vol.22, No.5, October, pp. 409-415.
Taal LA, Faber AW (1998) Post-traumatic stress, pain and anxiety in adult burn victims. BurnsVol 23, No.7/8, pp. 545-549.
Veterans Health Administration(2003)Management of Post-Traumatic Stress. Office of Quality and Performance publication. 10Q-CPG/PTSD-04. Washington, DC, VA/DoD Clinical Practice Guideline
Working Group, Veterans Health Administration, Department of Veterans Affairs and Health Affairs, Departmentof Defense. http://www.oqp.med.va.gov/cpg/PTSD/
Apprendre le protocole de la PEC du PTSD
